
Body composition is one of the variables evaluated during periods of training to be a concern for all practitioners, from those who would like to reduce body fat, who would like to maintain the composition and hypertrophy.
Although part of the routine especially professionals of physical education and sports nutrition, some details may interfere with the evaluation result. Thus we highlight some care must be taken to an accurate assessment, according to Heyward and Stolarczyk (1996):
Below we highlight the main methods of assessing body composition:
Direct Method: The dissection of corpses is the only methodology used directly; with this method is the separation of the various components of the human body in order to weigh and establish relations between them and the body weight. Because it is examining corpses, the method is rarely quoted. However, it is worth mentioning two studies that used the direct approach, the Matiegka (1921) and Drinkwater et al (1984).
Indirect methods
Hydrostatic weighing
Hydrostatic weighing is considered standard in other body composition analysis. This method is considered that the body is divided into two components, namely: fat mass and fat-free mass (Lukaski, 1987). Knowing the value of the body density, it is possible to estimate the percentage of body fat by means of mathematical models of Siri (1961) and Brozek et al. (1963). This method is rarely used and difficult to access.
Ray absorptiometry dual energy absorptiometry (DEXA)
The DEXA is a technique of “scanning” calculating the attenuation of x-rays that pass through the body (PAIVA et al. 2002). The subject is lying in anatomical
position and the x-ray is calculated by an energy detector. It is a noninvasive technique considered safe and separating the composition of three components: fat mass, fat-free mass and bone mass (CINTRA et al., 2004). The high cost and radiation exposure limits our capacity to use the technique.
Bioelectrical impedance analysis (BIA)
This method of driving by an electric current of low intensity the body. The impedance or resistance to electrical impulse is measured by bioimpedance. Lean body mass is a good conductor of energy by having a high concentration of water and electrolytes and fat mass a bad conductor of energy, it can be said that the impedance is directly proportional to the percentage of body fat (WAGNER and HEYWARD, 1999).
The validity and accuracy of the bioelectrical impedance method are influenced by various factors such as type of instrument, electrode placement, hydration level, diet, menstrual cycle, ambient temperature and equation predição.Assim, not to compromise the outcome of the body composition by bioelectrical impedance analysis, some previous care are important: do not eat or drink four hours before the test, do not exercise 24 hours before the test, urinate 30 minutes before the test, do not consume alcohol within 24 hours of the test and not have made use of diuretics in the last seven days (Heyward and Stolarczyk, 2000). Studies found a correlation between the method and the hydrostatic weighing (Wu et al. 1993) and the Dexa (Okasora et al (1999). The method can be interesting for body composition, as long as the care mentioned above are respected.
Body mass index
The BMI is calculated by dividing body weight in kilograms by height in meters squared. In studies with high population, BMI values are the most used for the analysis of body composition, but its interpretation in the individual context must be done with caution. The BMI is to estimate how much greater than the calculation result is, the greater the amount of body fat (GUEDES, 2006).
Despite being widely used, the method has shown some limitations. People with very high lean body mass because of the practice of physical exercise or very low due to some disease or accident, can alter the calculation without it can be calculated if there have been changes in lean mass or body fat.
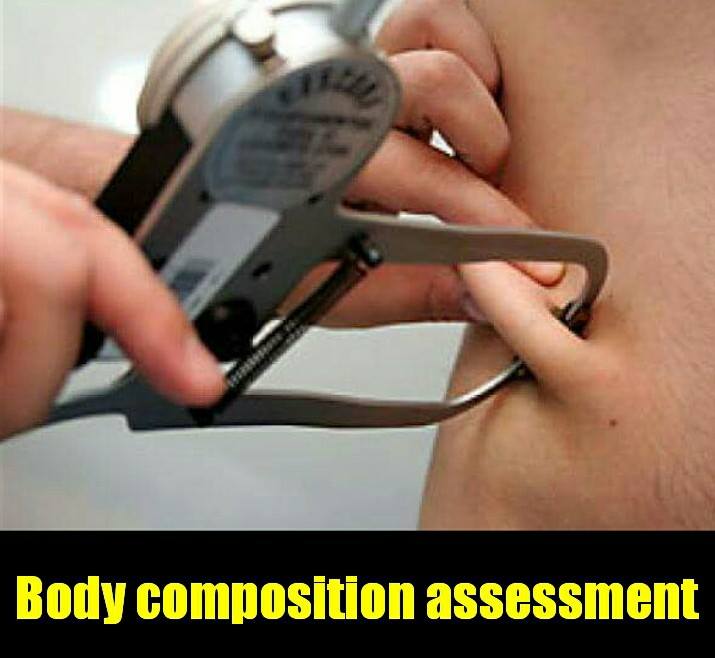
Skin folds
The higher proportion of body fat is located in the subcutaneous tissue and thus the measurement of their thickness is used as the amount of body fat indicator located in a particular region of the body. Due to fluctuations in body fat volume according to body region, it is required measuring the folds of various regions of the body to an appropriate calculation (GUEDES, 2006).
Due to its easy use and lower cost in comparison to other methods, the technique has been widely used for the calculation of body fat. The type of caliper used and the evaluator’s experience are crucial to an accurate assessment (GUEDES, 2006).
Some of the more equations used to calculate the percentage of body fat by skin folds are the proposals for Deurenberg et al (1990) that consider gender, ethnicity, age and sexual maturity (pre-pubescent or post-pubescent), and the equation proposed by Slaughter et al (1988), which are considered gender and ethnicity.
The method is advisable for smaller populations and has limitations in people with high body fat.
Measures perimeters
Perimeter measures more used in the evaluation of body composition in children are: waist circumference and waist / hip ratio. Concern about such measures of the greater risk to health related to fat accumulation in this region of the body, regardless of age and the amount of total body fat (THOMAS et al., 2004).
A major limitation to the use of waist circumference in children is the absence of a Recommended cutoff worldwide to evaluate the risk of developing cardiovascular and metabolic diseases.
Waist / height
The waist / height is calculated by dividing waist circumference (cm) by measuring the height (cm). Some authors emphasize the importance of this calculation to associate the result to cardiovascular risk factors in adults and children (LIN et al, 2002;. FREEDMAN et al., 2007). The waist / height is a key indicator to measure abdominal obesity and discriminates CHD risk better than BMI and waist circumference (LI et al., 2006). A higher value of 0.50 is suggested as the cutoff point for the risk of developing cardiovascular disease in individuals of both sexes from the age of six. Such a cut-off point can not be used for children under five years because studies show that this figure overestimates the risk of developing heart disease (SAVVA et al., 2000; HSIEH et al., 2003).